
Full-Thickness Scalp Wound in a Neonate: How Hydroconductive Dressings Help Treatment
Elizabeth Day Dechant, BSN, RN, CWOCN, CFCN
January 18, 2024
January 18, 2024
Keywords
Categories
Introduction
There is a paucity of literature regarding neonatal wound treatment. While it is widely accepted that neonatal wounds heal more rapidly than those of adults, topical dressing selection and care management are often based on provider preference and available resources. Lack of wound care knowledge among hospitalists has been reported as a barrier to optimal wound management.1
Some factors may lead to improved outcomes in neonatal wound healing. These elements include the involvement of wound treatment experts to guide and oversee wound care practices and the maintenance of a well-balanced formulary of topical products. The latter allows customization of care to meet each patient’s needs.1 To illustrate how these factors can achieve best outcomes for this population, this piece will present a case study demonstrating the rapid healing of a full-thickness scalp wound in a neonatal patient.
Hypochlorous Acid
Solutions containing pure hypochlorous acid have been shown to be effective and safe for use in the neonatal population. Pure hypochlorous acid is an antibacterial and antifungal wound and skin cleanser. It provides chemical debridement of nonviable tissue.1-4
Hydroconductive Dressings
Hydroconductive dressings are superabsorbent, making them a good choice for highly exudative wounds. Additionally, hydroconductive dressings have been shown to reduce bacterial load by up to 90%. Contraindications for use of hydroconductive dressings include active arterial bleeding.5
Case Study
A 1-month-old infant developed a large cephalohematoma secondary to birth trauma. As the cephalohematoma evolved, soft tissue damage became increasingly demarcated, and a full-thickness wound opened at the apex of the scalp, as seen in Figure A. Imaging was performed to ensure that there was no involvement of the bone or dura. Neurosurgeons and plastic surgeons assessed the wound and determined no indication for surgical intervention.
WOC Nurses evaluated the wound and established a plan of care that included daily dressing changes. At each dressing change, the wound was flushed gently with 20-40ml of pure hypochlorous acid solution in a luer-lock syringe.
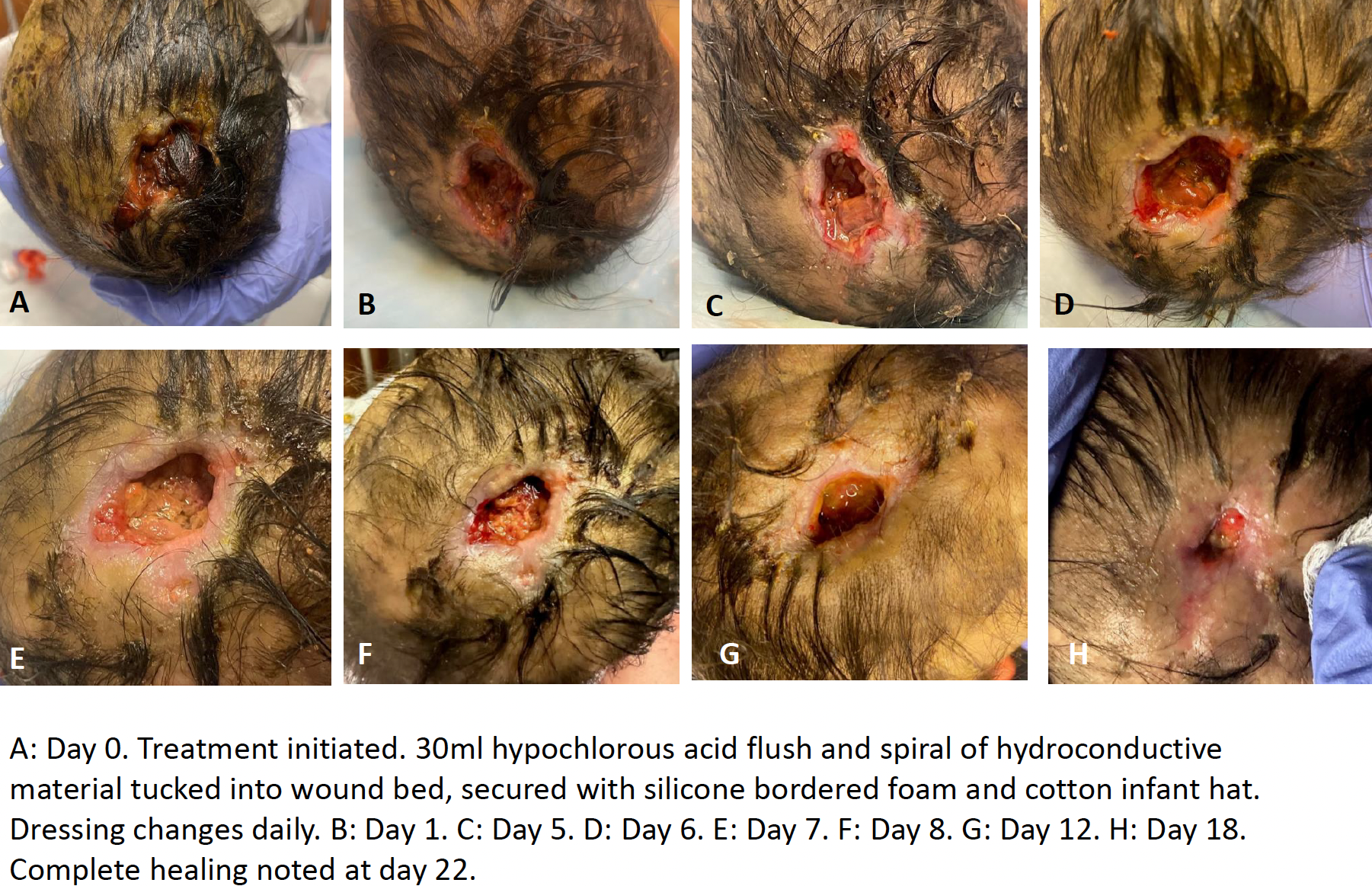
Nonviable tissue and debris were evacuated from the wound bed with each dressing change using this gentle flushing method. A small spiral of hydroconductive material was cut to fit the wound. The center of the spiral was gently tucked into the wound bed, with the remainder of the spiral filling the wound bed as possible and overlapping onto the periwound skin. Another piece of hydroconductive material was placed over this and secured with a silicone foam-bordered dressing. A soft cotton infant hat was used to further secure the dressing. The dressing did not adhere to the wound bed and removal was atraumatic at the time of each dressing change.
The infant tolerated dressing changes with minimal signs of pain. Pain was assessed by the patient crying and changes in vital signs. Pain medication was not administered before dressing changes. WOC Nurses performed the daily dressing changes Monday through Friday and bedside nursing staff performed dressing changes on weekends. As the wound decreased in size, the wound bed was noted to be increasingly clean and healthy appearing. Complete healing was noted after 22 days of treatment.
Conclusion
This case shows one example of a successful patient outcome resulting from optimal wound management and customization of care by wound treatment experts. Pure hypochlorous acid proved to be a safe and effective option for cleaning and flushing debris from the wound bed, while a custom cut hydroconductive dressing provided absorption of high levels of exudate. Skilled use of these advanced products and wound care techniques helped to facilitate rapid healing and prevent adverse sequelae, like wound infection or delayed healing.
References
- Dechant ED. Considerations for skin and wound care in pediatric patients. Phys Med Rehabil Clin N Am. 2022;33(4):759-771.
- Steen EH, Wang X, Boochoon K, et al. Wound healing and wound care in neonates: current therapies and novel options. Adv Skin Wound Care. 2020;33(6):294-300.
- Gozukucuk A, Cakiroglu B. Comparison of hypochlorous acid and Povidone Iodine as a disinfectant in neonatal circumcision. J Pediatr Urol. 2022;18(3):341.e1-341.e5.
- Elsass FT: Adjunctive debridement with hypochlorous acid for healing of complex wounds in children. Ostomy Wound Manage. 2016;62(4):14-16.
- Edwards-Jones V, Vishnyakov V, Spruce P. Laboratory evaluation of Drawtex Hydroconductive dressing with LevaFiber technology. J Wound Care. 2014;23(3):118, 120, 122-123.
About the Author
Elizabeth Day Dechant, BSN, RN, CWOCN, CFCN is a Certified Wound Ostomy Continence Nurse at Children’s of Alabama, where she provides wound treatment recommendations and wound management for both inpatients and outpatients with acute and chronic wounds. She provides staff education on skin and wound care, ostomy care, and pressure injury prevention. Elizabeth works diligently with the hospital’s Pressure Injury Prevention Team to track and reduce hospital-acquired pressure injuries.
The views and opinions expressed in this blog are solely those of the author, and do not represent the views of WoundSource, HMP Global, its affiliates, or subsidiary companies.





Follow WoundSource
Tweets by WoundSource