Advances in Hypochlorous Acid for Optimal Wound Care
May 1, 2026
Keywords
Categories
Hypochlorous Acid Mechanism of Action: Dual Antimicrobial and Debridement Effects
Therapeutic wound cleansing and debridement are two fundamental components of wound bed preparation that work synergistically for optimal wound healing.1-3 Integral debridement is a newly defined strategy that utilizes multiple debridement techniques over time as an individualized approach to traditional debridement, further optimizing wound bed preparation and wound healing outcomes by accounting for both patient and health care setting factors.3
Wound cleansing is an essential step before debridement to reduce the microbial load, remove any residual debris or contaminants, and prepare the wound bed. Following debridement, cleansing is also strongly recommended to promote a clean wound bed, minimize infection risk, and prevent any reformation of slough or biofilm.3 Although there are multiple options for wound cleansers, I prefer to use a pure hypochlorous acid (HOCl)-based cleanser before and after debridement for my patients with complex wounds.
HOCl is a naturally occurring, innate immune molecule produced by neutrophils as an oxidizing agent through the myeloperoxidase pathway during the respiratory burst.4 It exerts powerful, broad antimicrobial activity through rapid oxidative disruption of microbial cell membranes, protein denaturation, and DNA damage. The combined action of HOCl on multiple microbial cellular targets simultaneously inhibits microbial resistance.4 Furthermore, HOCl can penetrate and disrupt the extracellular matrix of biofilms as well as loosen slough via protonation to further support clinical debridement strategies, minimize inflammation, and potentially support tissue regeneration.3,5,6 As a reactive oxygen species that is naturally produced by neutrophils, HOCl demonstrates broad-spectrum efficacy with no known clinical bacterial resistance and results in minimal cytotoxicity to existing tissues at therapeutic concentrations and optimal pH.6,7 Taken together, these molecular properties make HOCl an attractive wound cleanser in my clinical practice, especially for patients with complex wounds.
Recent Advances of Hypochlorous Acid Solutions
In recent years, advances in HOCl wound cleansers have improved standard wound care. Chronic wounds are known to have an alkaline pH, which can allow microbial pathogens to thrive and may impede the healing process.8,9 Because wound healing is optimal in a slightly acidic environment with a pH between 3.5 to 5.5 that closely resembles the pH of healthy skin,8 cleansers formulated with pure HOCl at clinically appropriate pH, such as Vashe Wound Solution (Urgo Medical North America), are ideal for wound healing.7 At this optimal pH, protease activity and oxygen release are enhanced with reduced toxicity of bacterial end products, making it a safe and effective antimicrobial agent. Additionally, with minimal cytotoxic effects on existing tissue cells, there is increased fibroblast and keratinocyte activity, which promotes reepithelization and remodeling of the extracellular matrix as part of the wound healing process.10 Thus, pure formulations of HOCl at a targeted pH can maximize HOCl’s robust antimicrobial action, with no known contraindications, and better support the wound’s natural healing environment.
More recently, pure HOCl hydrogel formulations were developed to extend the benefits of HOCl liquid for more prolonged contact with the wound bed, which can be beneficial between dressing changes.11 A gel formulation, such as Vashe Antimicrobial Wound Ggl (Urgo Medical North America), provides a stable barrier with continuous moisture retention, promoting slough loosening and ultimately enhancing its role in wound bed preparation across a wide range of wound types.7 As a useful adjunct to sharp or other debridement methods, pure HOCl gel helps to keep wound surfaces clean and hydrated while maintaining robust antimicrobial activity.
Evidence-Based Clinical Incorporation of Hypochlorous Acid Solutions Into Standard Wound Care
Certain pure HOCl formulations are backed by peer-reviewed clinical evidence and guideline support, specifically in wound care settings.1,11-14 A gel formulation is now available and accessible that can provide additional and continuous antimicrobial benefits of HOCl, with consistent moisture management to enhance the wound-healing continuum of care and improve healing outcomes.11 Combining a skin-cleansing protocol with pure liquid HOCl, followed by application of HOCl wound gel before secondary dressing application, may provide the best dual-action protection to potentially simplify and standardize the wound cleansing process across a range of wound types.11 With no known contraindications or clinical resistance, a pure HOCl solution and gel duo addresses multiple wound-healing obstacles that can traditionally complicate patient management.
Clinical Results
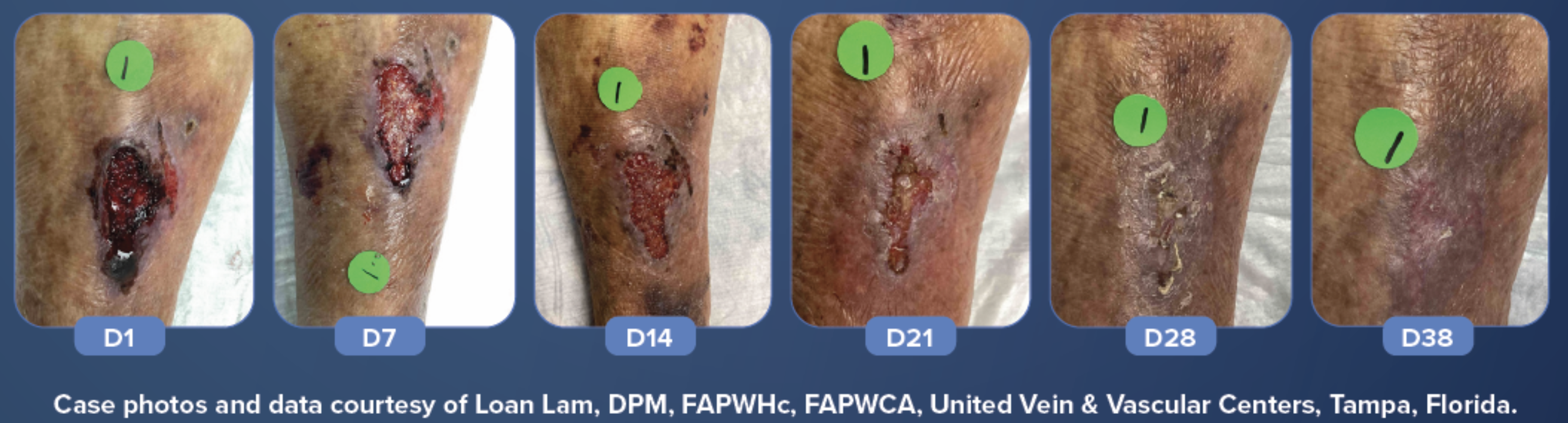
A non-diabetic, 80-year-old female with underlying chronic venous insufficiency presented to the treating clinician after a traumatic injury to her anterior leg that resulted in a wound. The patient was instructed to soak the wound daily with HOCl solution for 5 to 10 minutes, followed by application of Vashe Antimicrobial Wound Gel and wrapped with a conforming gauze roll. Dressings were changed daily.
Conclusions and Future Directions
Wound cleansing is an essential component of optimal wound management and healing. Advances in HOCl formulations make it an attractive cleanser and antimicrobial agent to support wound healing in conjunction with debridement techniques. For wound care professionals, incorporating these pure HOCl formulations into everyday use across a wide range of patients may standardize wound treatment and improve healing outcomes. Additional studies beyond case reports that demonstrate the safety and efficacy of the dual use of pure HOCl solution and gel will provide evidence for their combined use.
References
1. International Wound Infection Institute (IWII). Therapeutic wound and skin cleansing: Clinical evidence and recommendations. Wounds Int. 2025. https://woundsinternational.com/wp-content/uploads/2025/03/IWII_2025_Wound-cleansing-web-3.pdf
2. Sibbald RG, Elliott JA, Persaud-Jaimangal R, et al. Wound bed preparation 2021. Adv Skin Wound Care. 2021;34(4):183-195. doi:10.1097/01.ASW.0000733724.87630.d6
3. Mayer DO, Tettelbach WH, Ciprandi G, et al. Best practice for wound debridement. J Wound Care. 2024;33(Sup6b):S1-S32. doi:10.12968/jowc.2024.33.Sup6b.S1.
4. Haralović V, Mokos M, Špoljar S, Dolački L, Šitum M, Lugović-Mihić L. Hypochlorous acid: clinical insights and experience in dermatology, surgery, dentistry, ophthalmology, rhinology, and other specialties. Biomedicines. 2025;13(12):2921. Published 2025 Nov 28. doi:10.3390/biomedicines13122921
5. Robson MC. Treating chronic wounds with hypochlorous acid disrupts biofilm. Today’s Wound Clinic. 2014;8(9).
6. Day A, Alkhalil A, Carney BC, Hoffman HN, Moffatt LT, Shupp JW. Disruption of biofilms and neutralization of bacteria using hypochlorous acid solution: an in vivo and in vitro evaluation. Adv Skin Wound Care. 2017;30(12):543-551. doi:10.1097/01.ASW.0000526607.80113.66
7. Urgo Medical North America. Vashe Wound Solution. Accessed February 2026. https://www.urgomedical.us/products/vashe.
8. Nagoba BS, Suryawanshi NM, Wadher B, et al. Acidic environment and wound healing: A review. Wounds. 2015;27(1):5-11.
9. Sim P, Strudwick XL, Song Y, Cowin AJ, Garg S. Influence of acidic pH on wound healing in vivo: a novel perspective for wound treatment. Int J Mol Sci. 2022;23(21):13655. doi:10.3390/ijms232113655
10. Sakarya S, Gunay N, Karakulak M, Ozturk B, Ertugrul B. Hypochlorous acid: an ideal wound care agent with powerful microbicidal, antibiofilm, and wound healing potency. Wounds. 2014;26(12):342-50.
11. Herruzo R, Fondo Alvarez E, Herruzo I, Garrido-Estepa M, Santiso Casanova E, Cerame Perez S. Hypochlorous acid in a double formulation (liquid plus gel) is a key prognostic factor for healing and absence of infection in chronic ulcers. A nonrandomized concurrent treatment study. Health Sci Rep. 2023;6(10):e1497. Published 2023 Oct 25. doi:10.1002/hsr2.1497
12. Murphy C, Atkin L, Swanson T, et al. Defying hard-to-heal wounds with an early antibiofilm intervention strategy: wound hygiene. J Wound Care. 2020;29(Sup3b):S1-S26. doi:10.12968/jowc.2020.29.Sup3b.S1
13. Eriksson E, Liu PY, Schultz GS, et al. Chronic wounds: Treatment consensus. Wound Repair Regen. 2022;30(2):156-171. doi:10.1111/wrr.12994
14. Swanson T, Ousey K, Haesler E, et al. IWII Wound Infection in Clinical Practice consensus document: 2022 update. J Wound Care. 2022;31(Sup12):S10-S21. doi:10.12968/jowc.2022.31.Sup12.S10.
The views and opinions expressed in this content are solely those of the contributor, and do not represent the views of WoundSource, HMP Global, its affiliates, or subsidiary companies.

