Biopsy: Is it a DFU or Carcinoma? (And Why Does it Matter?)
April 14, 2023
Keywords
Categories
Introduction
Medical misdiagnosis is common and can be caused by errors in clinical reasoning that arise from knowledge deficits, cognitive biases, and dual-process thinking.1  Dual process thinking is a generally accepted conceptualization of clinical reasoning that includes an initial intuitive assessment followed by a slower logical analysis. Misdiagnosis can arise during both of these evaluative processes. For example, when we see a foot wound in a patient with diabetes and polyneuropathy, we default to assigning the diagnosis of diabetic foot ulcer (Figure 1).
Dual process thinking is a generally accepted conceptualization of clinical reasoning that includes an initial intuitive assessment followed by a slower logical analysis. Misdiagnosis can arise during both of these evaluative processes. For example, when we see a foot wound in a patient with diabetes and polyneuropathy, we default to assigning the diagnosis of diabetic foot ulcer (Figure 1).
As humans, we also default to truth or trust2; this contributes to misdiagnosis when the initial diagnosis is incorrect, especially if it is from a specialist, and we are less likely to question this conclusion. Regardless of their etiology, delayed and missed diagnoses continue to be a pervasive problem across care settings and specialties.3,4
Figure 1 shows squamous cell carcinoma to the anterio-lateral foot initially diagnosed as a diabetic foot ulcer. This injury was referred to a wound center from another wound provider.
When to Perform a Biopsy if Misdiagnosis is Suspected
 Astute wound clinicians are aware that the etiology of many chronic, hard-to-heal wounds are not actually what they initially appear to be. Over the course of treatment, alternative etiologies may be discovered, including cancer and autoimmune disorders such as pyoderma gangrenosum, vasculitis, sweet syndrome, or calcific arteriolopathy (calciphylaxis). When assessing patients and their wounds, findings that would raise suspicion for the need for wound biopsy, in my experience, include the following:
Astute wound clinicians are aware that the etiology of many chronic, hard-to-heal wounds are not actually what they initially appear to be. Over the course of treatment, alternative etiologies may be discovered, including cancer and autoimmune disorders such as pyoderma gangrenosum, vasculitis, sweet syndrome, or calcific arteriolopathy (calciphylaxis). When assessing patients and their wounds, findings that would raise suspicion for the need for wound biopsy, in my experience, include the following:
- Dimensions not improving as expected
- Concern for wound etiology
- Pain out of proportion to wound appearance,
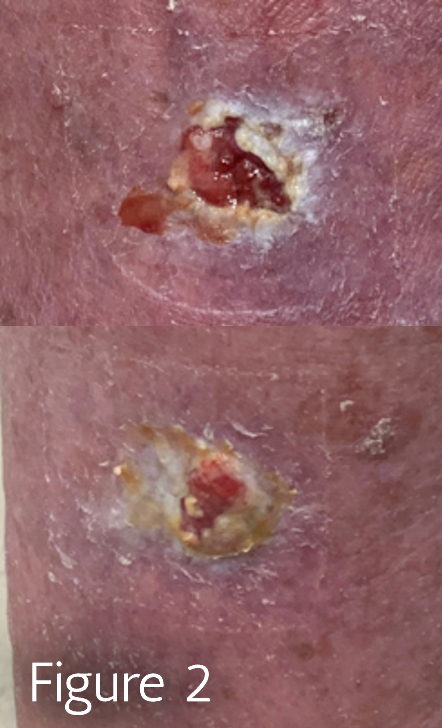
- An irregular wound base or borders (Figure 2)
In particular, Figure 2 shows Basal Cell Carcinoma to bilateral posterior lower legs that was initially diagnosed as venous leg ulcers and referred to a wound center from dermatology. In this injury, irregular, macerated edges are present. For these findings listed above, a punch biopsy of the newest lesion edge and intact tissue of the periwound can assist in diagnostic clarification.
If the reviewing laboratory has access to a dermatopathologist, a pathologist who specializes in skin, this is preferred as there would be more robust analysis with specialized testing techniques. It is important to include pertinent details in the dermatopathology order, including medical history findings associated with atypical skin lesions such as cancer, inflammatory bowel disease, or autoimmune disorders.
Squamous Cell Carcinomas: Avoiding Complications
Misdiagnosis of foot ulcers can lead to inappropriate plans of care and procedures that are contra-indicated in untreated cancerous lesions. Experts have frequently found squamous cell carcinomas (SCC) of the foot subject to inappropriate initial treatments, including debridement and cellular tissue product application.
One study of SCC of the foot found 75% of patients had received inappropriate or incomplete treatment of their cancer that eventually required more aggressive definitive treatment.5 Both cancer and impaired wound healing involve dysfunction of cell proliferation. In delayed wound healing, wound care professionals encourage cell division and proliferation through debridement. This treatment is especially indicated in diabetic foot ulcers to remove biofilm and senescent cells that accumulate in a hyperglycemic environment.6 Missed or delayed diagnosis of SCC in the diabetic foot can contribute to the use of interventions that increase the risk of encouraging tumor growth. Squamous cell carcinomas that arise in the setting of chronic wounds or scars are typically aggressive and are already associated with a poor prognosis.
A history of SCC should raise clinicians’ suspicion of wound etiology as recurrence after treatment is approximately 20-30%. Patients with skin cancers of the foot, such as SCC, benefit from continued multidisciplinary involvement. Patients who require definitive treatment for their SCC through wide local excisions or amputations may benefit from referral to the wound center for expedited treatment of their surgical wounds, given the risk for impaired wound healing in diabetes.6
Conclusion
Expanding our knowledge base is one of the best ways to reduce misdiagnosis and improve patient outcomes.2 Understanding the clinical presentation and disease course of atypical wounds assists providers in identifying suspicious findings and establishing the correct diagnosis to expedite healing.
References
- Norman GR, Monteiro SD, Sherbino J, Ilgen JS, Schmidt HG, Mamede S. The Causes of Errors in Clinical Reasoning: Cognitive Biases, Knowledge Deficits, and Dual Process Thinking. Acad Med. 2017;92(1):23-30. doi:10.1097/ACM.0000000000001421
- Gladwell M. Talking to Strangers: What We Should Know about the People We Don’t Know. Penguin Books; 2020.
- Balogh EP, Miller BT, Ball JR. Improving Diagnosis in Health Care. 2015.Washington, DC: National Academies Press.
- Institute of Medicine (US) Committee on Quality of Health Care in America, Kohn LT, Corrigan JM, Donaldson MS, eds. To Err is Human: Building a Safer Health System. Washington (DC): National Academies Press (US); 2000.
- Potter BK, Pitcher JD Jr, Adams SC, Temple HT. Squamous cell carcinoma of the foot. Foot Ankle Int. 2009;30(6):517-523. doi:10.3113/FAI.2009.0517
- Swoboda, L. & Held, J. Impaired Wound Healing in Diabetes. J Wound Care. 2022;31(10).
About the Author
Dr. Laura Swoboda is a Professor of Translational Science, Nurse Practitioner, and Wound Healing Coordinator at Froedtert & the Medical College of Wisconsin, where they advocate for nurse practitioners and nurse participation in research. They completed their Doctor of Nursing Practice degree at University of Wisconsin Milwaukee (UWM). Dr. Swoboda is a faculty member of the Clinical & Translational Science Institute of Southeast Wisconsin where they serve as principal investigator for quality improvement, evidence based practice, and research projects including the planning, implementation, management, and dissemination of projects in chronic wound care. They further participate in the research process in serving as a peer reviewer for scientific journals. Dr. Swoboda is on the National Pressure Injury Advisory Panel’s Prophylactic Dressing Standards Initiative Task Force, a member of the editorial board for the Wound Care Learning Network and Wound Management and Prevention, and on the board of directors for the WOCNCB and the AAWC.
The views and opinions expressed in this content are solely those of the contributor, and do not represent the views of WoundSource, HMP Global, its affiliates, or subsidiary companies.
More from this Author
// fixed missing link variable.
// fixed missing link variable.
// fixed missing link variable.