The Declining Rate of Diabetes-Related Complications
September 12, 2014
Keywords
Categories
By Michel H.E. Hermans, MD
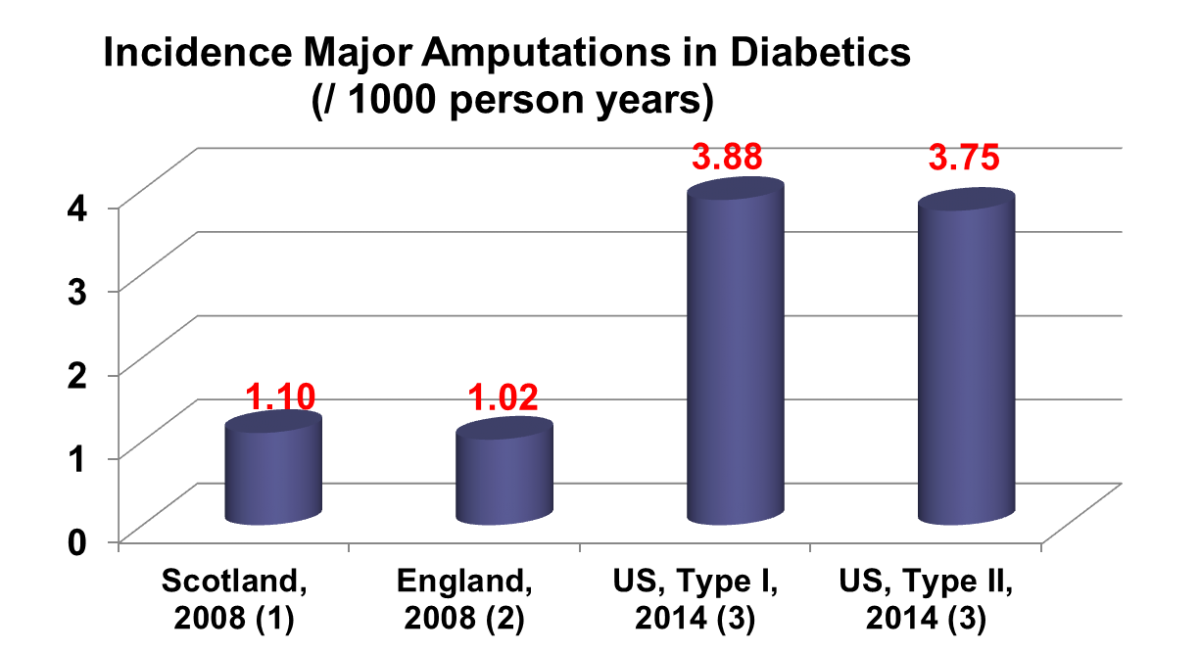
The CDC recently published encouraging data in the New England Journal of Medicine about a decline in the rate of five major complications related to diabetes mellitus: hyperglycemia, heart attack, stroke, kidney failure and amputations1. The report did not include eye-related problems (i.e. retinopathy, glaucoma, cataract). The rate of amputations went down from approx. +/- 55/10.000 adults (1990) to +/-26/10.000 adults (2010). The 2010 numbers on amputations are roughly in line with a more recent publication by the Agency for Healthcare Research and Quality (AHRQ) which reported an expected (2014) amputation rate of 3.75/person-year for type II and 3.8 for type I (figure I).
A Statistic That Remains Too High: Diabetes-Related Amputations
This is encouraging news, but the amputation rates are still high compared to some other countries: for example, 2008 amputation numbers for Scotland2 and England3, for both types of diabetes combined, were 1.10 and 1.02/1000 person years respectively. None of these data were specific about the type or level of amputation.
A reduction of about 50% in diabetes-related amputations sounds good, but cardiovascular complications and death from high blood sugar decreased by more than 60%. This seems to indicate that the efforts to prevent foot complications are not on the same level as the prevention of other complications. Edward W. Gregg, senior epidemiologist at the CDC and lead author of the article, in a New York times interview4 specifically mentioned the decline in smoking, the rising use of statins to lower cholesterol and the use of (better) medications to control blood pressure as factors contributing to the decline in (diabetes-related) heart attacks and strokes. There was no mentioning of specific measures to reduce the foot problems even more.
Diabetic foot ulcer prevention starts with some very basic measures, as implemented as part of her overall insurance in the case of a good friend of mine, living overseas. She suffers from diabetes mellitus type II and is largely blind. She gets visits every month by a specialized nurse who cuts her toenails, checks the skin on my friend’s feet and delivers the moisturizing creams my friend applies each day.
The Cost Diabetic Foot Ulcer Prevention Versus the Cost of Treatment
While this may sound as a (trivial) luxury, prevention is nearly always less expensive than treatment. The cost of a foot or lower leg amputation is estimated to be between $ 85,000 (Medicare) and $110,000 (Commercial insurance) and the cost of care for a diabetic foot ulcer without amputation is somewhere between $40,000 (Medicare) and $50,000 (Commercial insurance)5. Not even considering quality of life, prevention of ulcer formation in the first place would save the health care system a lot of money.
The Affordable Care Act allows for more screening for diabetes mellitus itself and other diseases. Hopefully, in a next round, it will also provide for preventative measures to avoid the development of a diabetic foot ulcer.
Sources
1. New CDC data show declines in some diabetes-related complications among US adults [news release]. Centers for Disease Control and Prevention; April 16, 2014. http://www.cdc.gov/media/releases/2014/p0416-diabetes-complications.html.
2. Kennon B, Leese GP, Cochrane L, et al. Reduced incidence of lower-extremity amputations in people with diabetes in Scotland: a nationwide study. Diabetes Care. 2012;35:2588-2590.
3. Holman N, Young RJ, Jeffcoate WJ. Variation in the recorded incidence of amputation of the lower limb in England. Diabetologia. 2012;55:1919-1925.
4. Tavernise S, Grady D. For Diabetics, Health Risks Fall Sharply. New York Times. April 16, 2014:A1.
5. Carls GS, Gibson TB, Driver VR, et al. The economic value of specialized lower-extremity medical care by podiatric physicians in the treatment of diabetic foot ulcers. J Am Podiatr Med Assoc. 2011;10193-115.
About the Author
Michel H.E. Hermans, MD, is an expert in wound care and related topics, trained in general surgery, trauma care and burn care in the Netherlands. He has more than 25 years of senior management experience in the wound care industry. He has conducted a large number of clinical trials relating to devices and drugs aimed at wound care and related indications and diseases. Dr. Hermans speaks internationally and has authored many published works relating to wound management.
The views and opinions expressed in this blog are solely those of the author, and do not represent the views of WoundSource, Kestrel Health Information, Inc., its affiliates, or subsidiary companies.
The views and opinions expressed in this content are solely those of the contributor, and do not represent the views of WoundSource, HMP Global, its affiliates, or subsidiary companies.

