
Diabetic Foot Ulcers and Pressure Injuries: How Do You Tell the Difference?
September 9, 2021
Keywords
Categories
In evaluating a patient with a wound on the foot, a question that often comes to mind is whether that wound is caused by pressure, diabetes mellitus (DM), ischemia, trauma, or a combination. For example, a patient with DM who happens to have an ulcer on the foot may have a diabetic foot ulcer (DFU) or possibly something else. One of the bigger challenges that many clinicians face is trying to determine the etiology of a foot ulcer. There has been a great deal of debate about DFUs and pressure injuries (PIs) on the feet of patients in terms of how to appropriately assess, classify, and treat them. The confusion and lack of evidence in differentiating between these two types of foot ulcers, particularly on the heel, can lead to misdiagnosis, which can increase both financial and patient-related costs.
Definitions of Pressure Injury and Diabetic Foot Ulcer
According to the National Pressure Injury Advisory Panel (NPIAP), a PI is “localized damage to the skin and underlying soft tissue usually over a bony prominence or related to a medical or other device. The injury can present as intact skin or an open ulcer and may be painful. The injury occurs as a result of intense and/or prolonged pressure or pressure in combination with shear.
The tolerance of soft tissue for pressure and shear may also be affected by microclimate, nutrition, perfusion, co-morbidities and condition of the soft tissue.” (The NPIAP has a staging system that was revised in 2016 and is beyond the scope of this article.1) The heel is the second most common site for the development of PIs, accounting for up to 28% of all PIs. A DFU is an open sore or wound on the foot of a person with DM, and it is most commonly located on the plantar surface, or bottom of the foot. There are numerous classification systems for DFUs that address anatomical involvement and the presence of any exposed structures and/or infection. DFUs occur in approximately 15% of persons with DM. Of those who develop a DFU, 6% will be hospitalized for infection or another ulcer-related complication. The risk of foot ulceration and limb amputation increases with age and the duration of DM.
Clinical Questions for Determining Etiology
It is obvious that there is overlap between definitions; however, taking a closer look at risk factors and clinical findings will establish an appropriate cause and can inform further treatment.
History: Is the patient diabetic? If so, then DFU is a possibility. In a patient who does not have DM and there is an index of suspicion, one may consider a hemoglobin A1c (Hgb A1c) test if the patient is over the age of 45 and has a body mass index >25 kg/m2. The Hgb A1c test is a diagnostic tool to screen for DM and can inform diagnostic choices. A patient with an elevated Hgb A1c (>6.4) should be referred to the primary care provider for further medical management.
Mobility: Is the patient ambulatory or has minimal mobility issues? Patients with decreased or limited mobility, hemiplegia, paraplegia, tetraplegia, decreased level of consciousness, or cognitive impairment may lack the ability to offload pressure to the feet, thereby increasing the risk for the development of PIs.
Neuropathy: Does the patient have a history of neuropathy or a loss of protective sensation? It is often said in the wound care community that “pain is the gift that no one wants.” In a patient with severe sensory neuropathy, an ulcer can easily develop if there is decreased or abnormal sensation to the foot. In such a case, patient may develop a full-thickness ulcer before even being aware that a problem exists. A monofilament examination is an easy way to identify whether loss of protective sensation is a factor. In general, patients with diminished pain responses as a result of neuropathy are more likely to be experiencing DFUs rather than PIs.
Foot deformities: Is there an obvious foot deformity? Many patients with DM have deformities such as Charcot foot in which the architecture of the foot becomes deranged and causes changes in pressure points in the foot. This, in turn, increases the risk of development of wounds related to DM.
Trauma: Is there a history of trauma? If so, what is the history of the trauma? Is it caused by a wound obtained during a transfer or by inadvertently stubbing the toe? Is it a wound caused by persistent forces on the foot during ambulation as a result of footwear or repetitive trauma?
History of previous amputations involving the foot: Is there a history of previous toe or partial foot amputations? This strongly suggests that the wound may be a DFU. Patients with previous amputations and history of DM are at significantly higher risk for the development of recurrent ulcers.
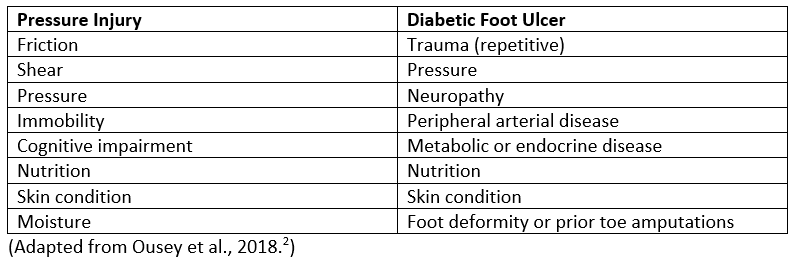
Factors Favoring Pressure Injury Versus Diabetic Foot Ulcer
Case Studies
 DFU in a 79-year-old diabetic man with surrounding cellulitis. This patient was ambulatory and living in the community until he noted a foul-smelling wound subsequent to donning a new pair of shoes. By the time he sought treatment, he had significant soft tissue infection with evidence of acute osteomyelitis noted on imaging. He was admitted to an acute care facility for antibiotic therapy and surgical intervention.
DFU in a 79-year-old diabetic man with surrounding cellulitis. This patient was ambulatory and living in the community until he noted a foul-smelling wound subsequent to donning a new pair of shoes. By the time he sought treatment, he had significant soft tissue infection with evidence of acute osteomyelitis noted on imaging. He was admitted to an acute care facility for antibiotic therapy and surgical intervention.

 Stage 4 PIs in a 54-year-old paraplegic man with a history of DM. This patient was an assisted living resident who lost his caregiver and was unable to turn and reposition himself appropriately. Although the patient has DM, his impaired mobility and inability to offload were significant factors in the development of his PIs. He also had limited access to resources and had protein-calorie malnutrition. Workup as an outpatient indicated no signs of infection. Home health care and social work services were ordered, as well as nutritional supplementation.
Stage 4 PIs in a 54-year-old paraplegic man with a history of DM. This patient was an assisted living resident who lost his caregiver and was unable to turn and reposition himself appropriately. Although the patient has DM, his impaired mobility and inability to offload were significant factors in the development of his PIs. He also had limited access to resources and had protein-calorie malnutrition. Workup as an outpatient indicated no signs of infection. Home health care and social work services were ordered, as well as nutritional supplementation.
Summary
In evaluating a foot wound, it is imperative to obtain a complete history and to perform a comprehensive evaluation to determine the etiology of the wound and factors contributing to its development. This information will, in turn, allow for a comprehensive plan of care for the patient to promote healing and to mitigate any factors that affect healing. This includes glycemic management when indicated, nutritional management, and control of any other comorbid conditions. In any patient with a lower extremity or foot wound, a vascular assessment is critical to determine perfusion status. Patients with impaired blood flow are at higher risk for complications associated with foot ulcers and will have challenges in terms of trying to heal.
References
1. Edsberg LE, Black JM, Goldberg M, McNichol L, Moore L, Sieggreen M. Revised National Pressure Ulcer Advisory Panel pressure injury staging system: revised pressure injury staging system. J Wound Ostomy Continence Nurs. 2016;43(6):585-597.
2. Ousey K, Chadwick P, Jawień A, et al. Identifying and treating foot ulcers in patients with diabetes: saving feet, legs and lives. J Wound Care. 2018;27(suppl 5):S1-S52.
Suggested Reading
Chan KS, Lo ZJ. Wound assessment, imaging and monitoring systems in diabetic foot ulcers: a systematic review. Int Wound J. 2020;17(6):1909-1923. Grimes J, Hall S, Holt G. Spot the difference: difficulties differentiating between pressure ulcers and foot ulcers. Diabetic Foot J. 2020;23(2):37-39. Diabetesonthenet.com. Accessed August 24, 2021. https://diabetesonthenet.com/wp-content/uploads/pdf/dotnb38087a2a24ddea…
Rayala BZ. Skin ulcers: Prevention and diagnosis of pressure, venous leg, and arterial ulcers. FP Essent. 2020;499:11-18. Remer EE. ICD-10 coding: diabetic foot ulcer or pressure ulcer? ICD10monitor.com. October 23, 2018, updated December 12, 2019. Accessed August 24, 2021. https://www.icd10monitor.com/icd-10-coding-diabetic-foot-ulcer-or-press…
Sorber R, Abularrage CJ. Diabetic foot ulcers: epidemiology and the role of multidisciplinary care teams. Semin Vasc Surg. 2021;34(1):47-53. Star A. Differentiating lower extremity wounds: arterial, venous, neurotrophic. Semin Intervent Radiol. 2018;35(5):399-405.
The views and opinions expressed in this content are solely those of the contributor, and do not represent the views of WoundSource, HMP Global, its affiliates, or subsidiary companies.
More from this Author
// fixed missing link variable.
// fixed missing link variable.
// fixed missing link variable.



