
How to Treat and Prevent Medical Device–Related Pressure Injuries
June 3, 2022
Keywords
Categories
How to Help Patients Protect the Skin They’re In
Medical device–related pressure injuries (MDRPIs) are recognized as a significant problem, evidenced by the inclusion in the National Pressure Injury Advisory Panel pressure injury definitions and described by Pitman and Gillespie in 2020.1 Prevention of medical device-related pressure injuries is a goal that may be achieved through meticulous patient care.
How to Treat a Medical Device-Related Deep Tissue Pressure Injury
One of the largest pressure injuries (PIs) I have seen was from a device-related pressure injury. The woman was only about 60 years old and had undergone a total hip replacement. When I came on for a late shift, she had been back on the medical-surgical unit for over 4 hours, and it appeared that she had not been repositioned at all. We had difficulty moving her and realized she had a wood block under her pelvis that allowed the x-ray plate to be slid in and out while in the operating room. We worked out that the wood block had been there for 6 hours. Her buttocks were raised about 2 inches by the block, and this would have increased the pressure.
On the side of her replaced hip, the corner of the block was digging in particularly hard. The skin there and across the sacrum was red, nonblanching, and obviously damaged. Over the next day or so, a deep tissue injury developed, and the skin peeled away. Instead of going home or to rehabilitation, she stayed with us for close to 2 weeks, during which time the wound developed depth and was surgically debrided. Pressure injuries from bed debris, such as a pair of glasses, intravenous caps (IV), dentures, ear buds, etc, are not uncommon. Such items dig into the skin and often cause odd patterns on the skin defined by the object.
How to Find the Cause of a Medical Device-Related Pressure Injury
It is not always obvious that the injury is pressure or device related. The following photograph is from a woman over 75 years old. She had diabetes that was poorly controlled with oral medication. She had visited her primary care provider 2 days before this picture was taken and had been prescribed a cephalosporin. There had been no traumatic injury to her foot that she could recall. She had claw toes with some neuropathy. Her foot was a little edematous, and the dorsalis pedis was palpable. There was minimal serous drainage, and she had no signs of infection and no fever. She had not had a nail on this toe for some time.

When asked for more detail on how the wound developed, the patient’s daughter described a fluid-filled blister that became purple. Initially, the health care professionals did not tie this to an event. When it was suggested to the patient and caregiver to see a vascular surgeon, they said that they had just had an appointment for some tests 10 days earlier. This was the “aha!” moment. The fluid-filled blister occurred 2 days after the visit. and yes, “come to think of it, they put a miniature blood pressure cuff around her toes” (to perform toe pressures)! The vascular service was called, and a follow-up appointment was made. A copy of this photograph was sent to them. A simple Xeroform dressing was applied by the daughter every other day, and the wound went on to heal, with no further complications. The testing had been done by a medical assistant, and despite some requests for information, it was not discovered whether any kind of mitigation had been performed. It is not known whether the patient and her family followed through with a formal complaint.
What Are the Major Causes of Medical Device-Related Pressure Injury (MDRPI)? Casts and Splints
Casts and splints are major causes of medical device-related pressure injuries. There are 2 main factors for this:
- When the order states that the device must not be removed
- When clinicians are worried about their competency to remove a splint and replace it correctly
Splints and casts that injure patients should be removed, preferably with the knowledge of the ordering physician. This is not always as easy as it sounds because doctors can be difficult to track down, and some splints seem impossible puzzles. If a cast needs removal when there is a “do-not-remove” order and the prescribing physician is unable to be contacted, an x-ray study should be done, and a suitable plan for fixation or treatment after cast removal should be devised. If a cast is then replaced, windows can be cut to allow wound inspection and dressing changes, or the cast can be bivalved to allow for regular removal.
Medical Device-Related Pressure Injury: Nonremovable Cast
The following photograph is of a 23-year-old male patient who had experienced a head injury and ankle fracture. There was a do-not-remove cast order in his chart on admission to rehabilitation, and the cast had been on for 2 weeks. There was considerable odor, and the cast was soiling the sheets. The cast was removed, revealing wounds medially and laterally. This photograph was taken several weeks later as the wounds were healing in a fresh bivalved cast that was removed every 3 days.

Prevention of Medical Device-Related Pressure Injury
How to: Nasogastric Tube (NG Tube) Placement
Nasogastric tubes (ng tubes) can cause significant pressure injuries. Securing ng tubes can be challenging, and the method shown here for placement that is recommended by the American Association of Critical Care Nurses is very effective. It does not force the ng tube onto the skin and allows sufficient, comfortable movement. The method used in intensive care unit in the United Kingdom does not split the end of the part that goes around the ng tube. Manufacturers make rather bulky devices that are better than other tape methods of placement. It is unfortunate that no company has made this simple, effective tape technique available.
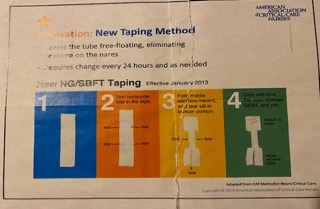
Method of nasogastric (NG) tube and small-bore feeding tube (SBFT) taping. (Copyright 2014, American Association of Critical Care Nurses.)
The infographic on nasogastric tube placement above reads: Innovation: New Taping Method Leaves the tube free-floating, eliminating pressure on the nares Requires change every 24 hours and as needed New NG/SBFT Taping (effective January 2013)
- Lay out the tape.
- Tear horizontal slits in the tape
- Fold middle sections inward, and tear slit in bottom portion. (Note: the slit in the bottom portion will wrap around the tube and the top portion will attach to the nose.)
- Date and time the tape, change Q24H, and pm.
How to Prevent Medical Device-Related Pressure Injuries: 10 Tips
Preventing medical device-related pressure injuries is better than treating these injuries. Prevention saves both patients and health care professionals time, resources, and discomfort. As seen the previous case studies, medical device-related pressure injuries can result in longer hospital stays for patients, not to mention detective work for health care professionals to find the origin of the injury. Here are 10 hints and tips to assist in preventing medical device-related pressure injuries:
- Avoid working from the bed. If it is necessary, use a defined space (a disposable underpad), so intravenous caps and other equipment do not stray under the covers or the patient.
- When turning a patient, always check that the sheet is smooth under them; this ensures their bed is clear of glasses, dentures, books, crumbs, and intravenous caps.
- Every time the patient is repositioned, “clear the skin.” This means all tubes head to toe need to be lifted free from the skin and repositioned optimally for comfort and safety. Tapes and supports for tracheostomy and endotracheal tubes may need to be dried or changed. Staff performing such care need to be confident and competent or work with a more experienced colleague.
- Oxygen tubing may need to be softer for patients with more delicate skin, and when crossing the ear, soft foam covers can be used or hydrocolloid cheek or face supports can be placed.
- Tubes that need to be very securely fixed to the skin (such as intravenous lines, arterial catheters, and chest drains) should have fixation methods used that will not overpressurize the skin and fully support the device.
- Urinary catheters should be secured in a way that allows repositioning of the tubing after moving the patient (a strap that can be moved from one leg to another may be preferable to an adhesive patch).
- For a splint that can be removed fully, take care to note how it is placed before removing it (take a photograph if necessary). Knowing how the splint is meant to function will help to ascertain correct positioning. At handover, show the incoming colleague the device and assist with repositioning it; ask a therapist to assist. Ensure the patient is comfortable and that the splint “feels right.”
- Some splints and casts cannot be removed or do not need to be removed every time a patient is repositioned. These should be checked visually to ensure they are not chafing the skin. Clearing the skin at the border of the cast and drying any moisture buildup promote comfort. It may be necessary to use clothing material or padding to ensure that padding will redistribute pressure over a wider surface and not increase it. Make sure anything used for padding cannot “get lost” and “slip” into the cast. If a problem is identified, discuss with colleagues how to address the issue. If an order to not remove a cast is received, have the order updated to include criteria and action needed if removal is necessary (pain, fever, drainage, changes in skin perfusion, etc).
- Offloading boots need to be removed during repositioning, and the skin must be checked before replacing the boots after repositioning.
- If the patient has lower extremity arterial disease or neuropathy, a bed cradle may be needed to offload bedclothes and prevent pressure on the toes.
Patient Involvement in Medical Device-Related Pressure Injury Prevention
Education relating to medical devices, splints, and casts tends to be from staff on the unit. This education is most often utilized if a patient is on maternity and has a knee brace. Often, it is the patient who is likely to be more familiar with the device than the nurse. Asking the patient should not be viewed as a problem and is preferable to patient repositioning of the device afterward. Medical device procurement must include staff involvement with medical device purchasing so that company rhetoric and cost are not placed above patient comfort and safety or staff experience and expertise.
Conclusion
The prevention of medical device-related pressure injuries is very much the responsibility of the whole health care team, and nurses need to involve and corral them all. The patient’s plan of care can’t include every action needed to prevent device-related injury. Caregivers need to make it routine to smooth sheets, “clear the skin,” and move and secure all tubes. This is Care. Do-not-remove orders for splints and casts need to be clarified, and staff need to feel competent and confident to manage devices needed for patient care and treatment. We need to protect the patient and the “skin they are in.”
Reference
- Pitman J, Gillespie C. Medical device-related pressure injuries. Crit Care Nurs Clin North Am. 2020;32(4);533-542.
About the Author
Margaret Heale has a clinical consulting service, Heale Wound Care in Southeastern Vermont and draws on her extensive experience as a wound, ostomy and continence nurse in acute and long-term care settings to provide education and holistic care in her practice.
The views and opinions expressed in this content are solely those of the contributor, and do not represent the views of WoundSource, HMP Global, its affiliates, or subsidiary companies.
More from this Author
// fixed missing link variable.
// fixed missing link variable.
// fixed missing link variable.




