Chronicity in Lower Extremity Wounds
Practice Accelerator
February 28, 2021
February 28, 2021
Keywords
Categories
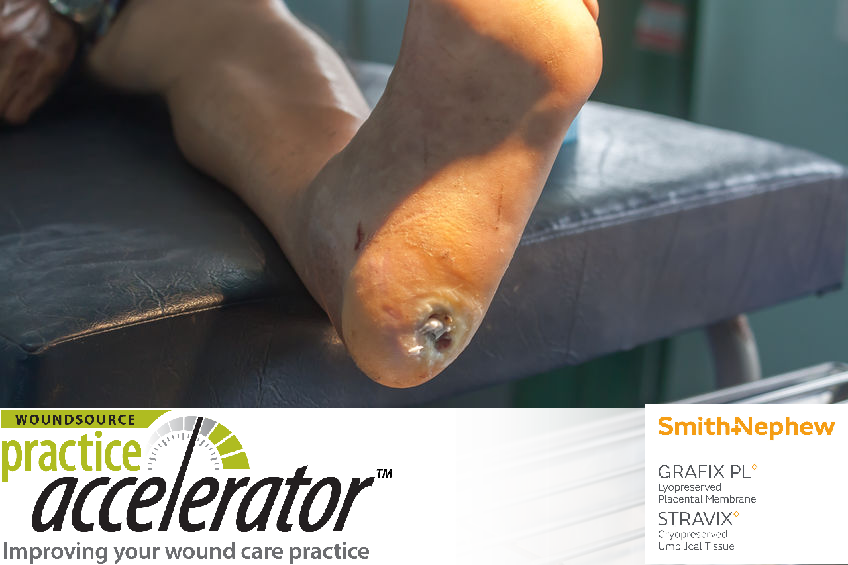
Chronic wounds of the lower extremities impose an increasing burden on health care providers and systems, and they can have a devastating impact on patients and their families. These wounds include diabetic ulcers, venous ulcers, arterial ulcers, and pressure injuries. The estimated socioeconomic cost of chronic wounds is 2% to 4% of the health budget in Western countries. Moreover, patient mortality in individuals with chronic wounds has been estimated at 28% over a two-year period, significantly higher than the 4% mortality rate reported for 75 to 79 year-olds without chronic wounds.1 Chronic wounds are commonly defined as those that fail to proceed through an orderly and timely process to produce anatomic and functional integrity.2 Despite differences in etiology, chronic wounds share many features, including excessive levels of proinflammatory cytokines, persistent infection, formation of drug-resistant microbial biofilms, and senescent cells that do not respond to reparative stimuli.3
How much do you know about complex wounds? Take our 10-question quiz to find out! Click here.
Contributors to Wound Chronicity
Many factors can contribute to wound chronicity, including:
Devitalized tissue: The presence of nonviable or necrotic tissue provides an optimal environment for the multiplication of microorganisms that can prolong the inflammatory phase of healing and even induce infection. Slough found on these wounds often contains fibrin, pus, leucocytes, microorganisms, and proteinaceous materials, all of which can lead to increased bioburden.1
Bioburden: Biofilms on chronic wounds, including bacteria, fungi, and other microorganisms, aggregate to form colonies that are encapsulated in extracellular polymeric substance. This substance provides a protective barrier against the host’s immune response and makes the microorganisms tolerant to antimicrobial agents.4 Biofilms can also stimulate inflammatory responses, which increases edema and exudate.1
Comorbidities: The presence of certain conditions can increase the likelihood of wound recurrence and chronicity. The most common comorbidities reported include diabetes, peripheral vascular or arterial disease, hypertension, and peripheral neuropathy. Less common comorbidities include renal disease, effects of immunosuppressive therapy, connective tissue disorders, reception of a transplant organ, and human immunodeficiency virus.5
Social factors: Certain elements of the patient’s social context can also contribute to delayed healing. These factors include occupational status, access to health care services, nutritional habits, and fiscal resources.5 Body mass index, smoking status, age, sex, race or ethnicity, and other concomitant medical conditions can also impact wound healing and contribute to chronicity.6
Managing Chronic Wounds
Initially, all chronic wounds should be treated according to the TIMERS principle, which includes:
- Tissue management: Remove necrotic or compromised tissue to ensure a viable wound base. Debridement may be repeated several times with chronic wounds.7
- Inflammation or infection: Infection and inflammation are known to impair healing. Controlling the bioburden, or the presence and concentration of bacteria and fungal organisms, can optimize the wound bed conditions.8 Bioburden can be controlled through debridement and antimicrobial agents.3
- Moisture balance: Creating a balanced moisture level through selection of proper dressings is instrumental in promoting re-epithelialization.2 Moist wounds heal more quickly and have less risk of infection, although drainage needs to be controlled and kept off the periwound.3Edge (epithelial) advancement: Chronic wounds frequently do not progress sequentially through the phases of healing. Any treatment selected should work to promote epithelialization, control epibole, and achieve a healthy periwound area.8
- Regeneration or repair: Focus on wound closure by providing a matrix to support cell infiltration, and stimulate cell activity using signal molecules or growth factors, delivery of oxygen, use of negative pressure wound therapy, or application of stem cells.9
- Social factors: Use a holistic approach to assessing and treating a chronic wound and increase patient engagement.9
After these general measures have been taken to promote healing of a chronic wound, additional treatments may be indicated by the type of lower extremity wound. For instance, patients with arterial ulcers should be referred to a vascular surgeon; those with venous ulcers should compress and elevate the limb and exercise if they are able, and those with diabetic foot ulcers may elevate the foot and treat underlying peripheral arterial disease.

References
- Galea E, Khatib M. Addressing wound chronicity factors: UrgoClean Ag and UrgoStart case studies. Wounds Middle East. 2020;7(1):25-29.
- Martinengo L, Olsson M, Bajpai R, et al. Prevalence of chronic wounds in the general population: systematic review and meta-analysis of observational studies. Ann Epidemiol. 2019;29(8):8-15.
- Bowers S, Franco E. Chronic wounds: Evaluation and management. Am Fam Physician. 2020;101(3):159-166.
- Bjarnsholt T, Eberlein T, Malone M, Schultz G. Management of wound biofilm made easy. Wounds Int. 2017;8(2):1-6.
- Murray RZ, West ZE, McGuiness W. The multifactorial formation of chronic wounds. Wound Pract Res. 2018;26(1):38-46.
- Kim PJ, Attinger CE, Orgill D, et al. Complex lower extremity wound in the complex host: results from a multicenter registry. Plast Reconstr Surg Glob Open. 2019 7(4):e2129. https://doi.10.1097/GOX.0000000000002129.
- Falanga V. Wound bed preparation: science applied to practice. In: Calne S, ed. Wound Bed Preparation in Practice. European Wound Management Association (EWWA). London, United Kingdom: MEP Ltd; 2004.
- Moore Z, Dowsett C, Smith G, et al. TIME CDST: an updated tool to address the current challenges in wound care. J Wound Care. 2019;28(3):154-161.
- Stevenson P, Schultz G. 2019 international consensus includes biofilm treatment as new standard of care. Wound Manag Prev. 2019;65(7).
The views and opinions expressed in this content are solely those of the contributor, and do not represent the views of WoundSource, HMP Global, its affiliates, or subsidiary companies.
More from this Author
// fixed missing link variable.
// fixed missing link variable.
// fixed missing link variable.




